| |
Ovarian Cysts and Tubal Cysts
A cyst is a 'space containing fluid'. Simple cysts have thin walls. Complex cysts contain both fluid and solid spaces, as seen on High Definition Ultrasound scans. NB: Not all scans, like surgery are equal.
Physiological
 Associated with ovulation (eg corpus luteum=yellow body) which resolve Associated with ovulation (eg corpus luteum=yellow body) which resolve
over weeks
Pathological
Polycystic Ovaries - rarely requires surgical drilling or excision
Benign Cysts
Endometrioma's (associated with endometriosis) require removal to improve fertility and pelvic pain. Often associated with moderate or severe endometriosis, Ultrasound scans are unable to detect subtle changes. They are often associated with modest elevation of CA 125
Serous or Mucinous Cysts require removal by excision (not drainage)
and have an ongoing risk of recurrence (>10%)
Dermoid Cysts Mature teratoma are uncommon and contain embryological remnants (hair, teeth etc) and require complete careful excision by laparoscopy
Tubal cysts
Malignant Cysts If ever confirmed require tertiary treatment by Oncologist.
Epithelial Ovarian Cancer presents most often after menopause. Where Ultrasound scan features include abnormal projections, blood supply, complex spaces and free fluid in the pelvis, etc. May be associated with HIGH CA125 levels.
Germ Cell and Stromal Cell Cancer has many sub-types, and useful markers for some of these cancers
Borderline Ovarian Tumours
For appointments with Dr Simon Gordon |
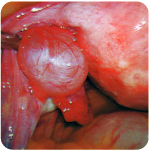 |
Tubal cyst |
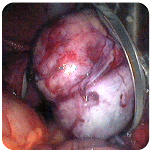 |
Endocatch to remove 10cm Dermoid cyst |
|


